
*IV Ketamine, NR, and NAD+ have been used clinically off-label for decades. They are not FDA approved for the treatment of any psychiatric or pain condition. All medical treatments carry risks and benefits that you must discuss with a doctor at Clarus Health to learn if these therapies are right for you.

If your mood falls apart in the second half of your cycle, or perimenopause brought a heaviness that antidepressants never lifted, you know the link between low progesterone and depression is real. Most of what you find online reduces it to a simple equation where low progesterone causes depression and topping your levels back up resolves it. But that doesn't explain why some women feel much worse when taking progesterone. Dr. Kaveh explains the low progesterone-depression link.
Low progesterone symptoms overlapping depression
Low progesterone symptoms are often misinterpreted or gaslit. Mood changes, anxiety, and depression are all recognized signs of low progesterone, which is why these symptoms so often get taken to a therapist or a psychiatrist instead:
- Mood swings, irritability, or a short fuse that isn't like you
- Low mood or a flat, heavy feeling in the two weeks before your period
- Anxiety that arrives on a schedule
- Insomnia, or waking at 3 a.m. and not getting back to sleep
- Brain fog and trouble concentrating
- Fatigue that sleep doesn't fix
The physical low progesterone symptoms usually arrive alongside these, and the Cleveland Clinic lists the familiar ones: irregular or shorter cycles, spotting between periods, headaches, low libido, and difficulty conceiving. Breast tenderness and heavier or less predictable bleeding are common, as well. When mood symptoms and cycle symptoms show up together like this, hormones deserve a place in the conversation, though in practice they rarely get one.
The proof that low progesterone and depression are connected
The clearest evidence comes from perimenopause. Researchers tracking women through the transition found that those who had stopped producing ovulatory levels of progesterone scored significantly higher for depression - and the link held even after accounting for weight, past depression, and life stress. Swinging estrogen made mood worse independently, which is why perimenopause feels less like a slow fade and more like a roller coaster.
Your mood changes in your 40's may be biological
Why progesterone controls your mood in the first place
Progesterone shapes your mood largely through what your body converts it into.
Progesterone becomes allopregnanolone, which switches on the brain's main calming system - the same target as anti-anxiety medication. When that pathway falters, mood, anxiety, and sleep go with it.
A strong signal came from the FDA. In 2023 it approved a synthetic analogue of allopregnanolone as the first pill for postpartum depression. Postpartum depression is believed to happen after progesterone and allopregnenolone levels plummet after childbirth. Women who take it can improve within days, and the fact that a federal regulator reviewed the evidence and signed off tells you how seriously this hormone pathway affects mood.
Why "just take more progesterone" backfires
This is where the internet's advice gets women into trouble, and why so many feel worse on drugstore progesterone cream.
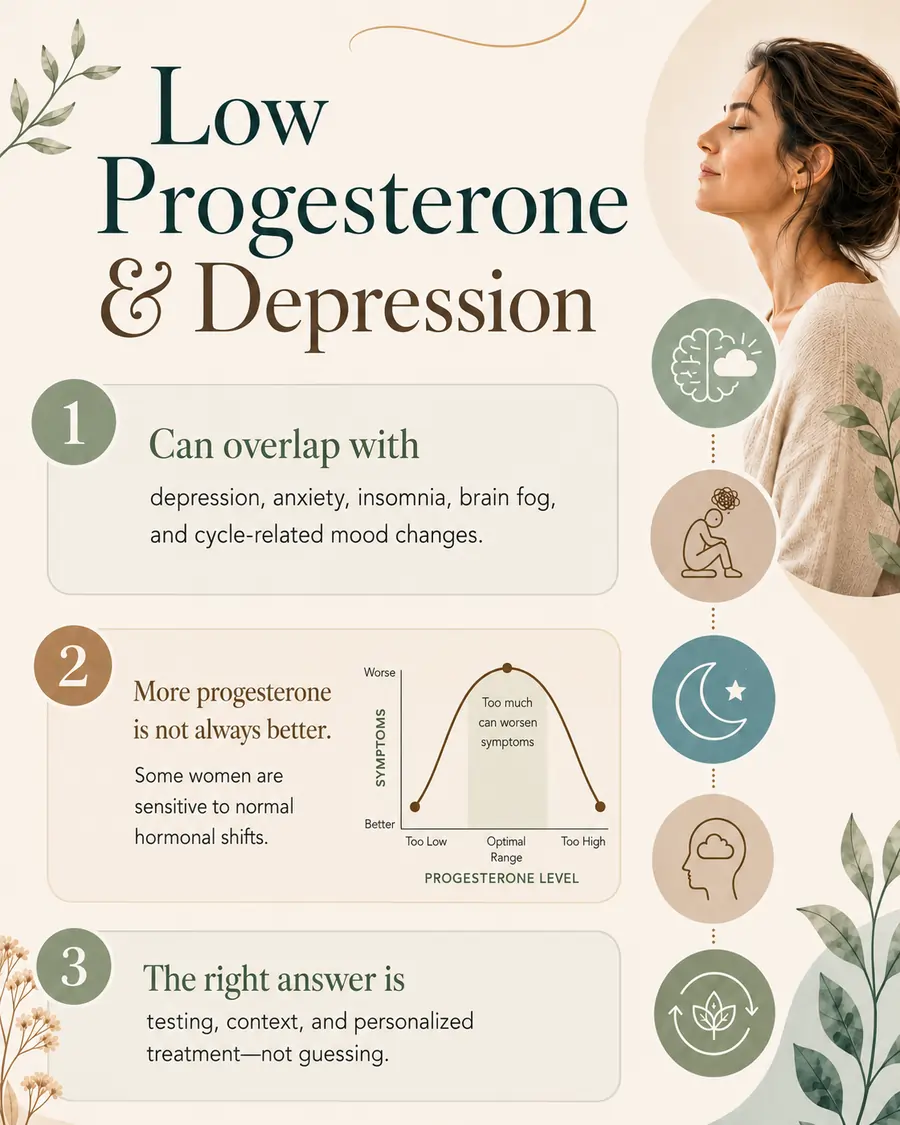
Raising your levels does not reliably improve your mood. The response to this pathway follows an upside-down U, meaning that in sensitive women the levels producing the worst mood are the ordinary ones found in a normal cycle, while very low and very high levels affect mood far less. Push a susceptible woman straight into that middle zone and you can manufacture the exact irritability and low mood she was trying to escape.
With PMDD, in particular, low levels are not even the underlying issue. Some premenstrual symptoms do not come from having too little progesterone, because hormone levels look much the same in women with symptoms and women without. What separates them is sensitivity, meaning how your particular brain reacts to normal hormonal shifts.
Because two women can have identical lab results and completely different symptoms, low progesterone symptoms need a physician who can read them in context rather than a product over the counter
If hormones made you feel worse before, you may have been given the wrong one
Synthetic progestins - what's in most conventional prescriptions and birth control - can flatten mood, because they shut down your own ovulation and can't be converted into allopregnanolone. You lose the calming metabolite and keep everything else.
Bioidentical progesterone is structurally identical to what your body makes, so it can travel that pathway. If you've been told hormones made your depression worse, there's a real chance you were simply given the wrong molecule.
How we treat low progesterone symptoms and depression together
We test before we treat. That means full hormone testing - progesterone, estrogen, testosterone, DHEA, cortisol, thyroid - at the right time of your cycle, plus genetic markers that shape how you process hormones. Normal-looking labs don't mean your hormone balance is healthy: your symptom pattern matters as much as the numbers.
When the picture is hormonal, bioidentical hormone therapy is dosed to your biology and adjusted to how you actually respond.
When depression runs deeper than the hormones, we treat it directly. Clarus Health offers IV ketamine, Spravato (FDA-approved and insurance-covered), and the Stellate Ganglion Block for depression that hasn't responded to conventional treatment, delivered by Stanford- and Harvard-trained physicians.
Many women need hormones balanced and depression treated at the same time, which is exactly why we do both in one team rather than splitting care teams.
Is low progesterone affecting your mood?
If your depression follows your cycle, showed up with perimenopause, or never fully responded to antidepressants, low progesterone may be part of your story - and the solution is to work with a hormone specialist. Schedule a free consultation and to find out.


