
Estrogen cream: is it actually safe?
Estrogen cream is popular, but is it safe? Learn how it can help UTIs, dryness, itching, and vaginal atrophy with manageable risks (under doctor supervision)
*IV Ketamine, NR, and NAD+ have been used clinically off-label for decades. They are not FDA approved for the treatment of any psychiatric or pain condition. All medical treatments carry risks and benefits that you must discuss with a doctor at Clarus Health to learn if these therapies are right for you.

Estrogen cream: is it actually safe?
Estrogen cream is very popular — but not all estrogen creams are the same. The type, where it's applied, and how it's absorbed determine everything about its safety profile.
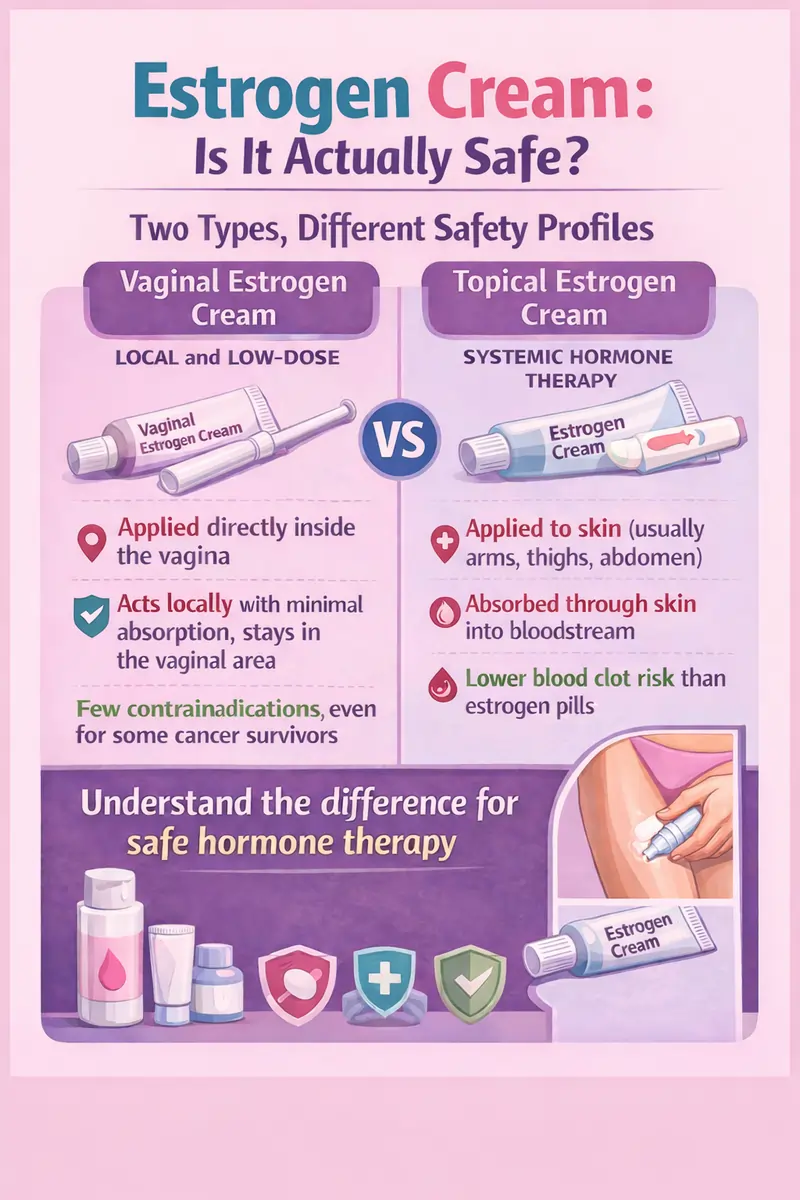
When patients ask me about estrogen cream, they're usually referring to one of two things: a vaginal estrogen cream for menopause symptoms, or a topical estrogen cream applied to the skin for systemic hormone replacement. These are not the same product! They don't work the same way, and they don't carry the same risks - here's what you need to know about different estrogen creams.
Vaginal estrogen cream: the local option
Vaginal estrogen cream is applied directly inside the vagina to treat Genitourinary Syndrome of Menopause (GSM) — dryness, irritation, pain with intercourse, and recurrent urinary tract infections (UTIs). Common examples are Estrace and Premarin Vaginal Cream.
What do these estrogen creams do? Vaginal estrogen cream acts locally, not systemically. Low-dose vaginal preparations keep serum estradiol levels within the postmenopausal range — meaning minimal whole-body exposure. This is why vaginal estrogen cream has very few contraindications and can be appropriate even for many breast cancer survivors (but you must always discuss this with your oncologist first).
Topical estrogen cream: the systemic option
Topical estrogen cream is applied to the arms, thighs, or abdomen. This is "body-wide" estrogen delivery. It absorbs through the skin directly into the bloodstream, bypassing the liver entirely. That liver bypass makes it typically safer than oral estrogen pills. Bypassing the liver helps substantially lower blood clot risks than estrogen pills.
As part of a well-designed bioidentical hormone replacement therapy (BHRT) plan, topical estrogen cream is often the delivery method of choice for women who want systemic relief without the oral estrogen risk profile, or who simply prefer a cream to a patch.
What estrogen cream actually treats well
Genitourinary syndrome of menopause (GSM): estrogen cream works very well
Vaginal estrogen is the most effective treatment for GSM. Multiple studies have found vaginal estrogen formulations - creams, tablets, rings - effective for these irritating, and sometimes dangerous, symptoms. Most women see meaningful improvement within a few weeks.
Recurrent UTIs also benefit from estrogen cream
Declining estrogen alters vaginal pH and disrupts the urinary tract's protective environment, making postmenopausal women significantly more prone to recurrent infections. Vaginal estrogen cream restores the vaginal lining and pH, reducing UTI frequency and helping patients avoid repeated antibiotic courses - a meaningful benefit that often goes underdiscussed.
Hot flashes and systemic menopause symptoms: this needs systemic estrogen cream
Topical estrogen cream applied to the skin is effective for hot flashes, night sweats, mood instability, and sleep disruption - comparable in efficacy to patches and pills. The advantage over pills is the liver bypass and reduced clotting risk. For some women, it's also simply more convenient than an adhesive patch. Consistent dosing matters more with cream than patches, which release a controlled amount automatically.
Estrogen cream and blood clot risk
Oral estrogen undergoes first-pass liver metabolism, triggering increased clotting factor production - this can increase blood clot and stroke risk. Topical and vaginal estrogen cream, absorbed through the skin or acting locally, bypass the liver entirely.
A meta-analysis of 15 studies found oral estrogen associated with a 63% higher VTE risk and more than double the DVT risk compared to transdermal estrogen. Transdermal estrogen's pooled risk ratio was 1.0 — no meaningful elevation above baseline.
The ESTHER study in Circulation found oral estrogen carried a fourfold increased blood clot risk while transdermal showed none. A 2025 systematic review confirmed that transdermal estrogen confers no increased VTE risk even in women with existing risk factors. For vaginal estrogen cream specifically, the Nurses' Health Study found no association with cardiovascular disease, breast cancer, or endometrial cancer.
What about estrogen cream for skin aging?
Estrogen loss after menopause contributes to collagen loss, thinning, and dryness. But most studies on estrogen face creams are small, short-term, and can't isolate estrogen's contribution from other ingredients. For women with a uterus, estrogen absorbed through facial skin can raise endometrial risk without progesterone protection if body-wide levels rise meaningfully.
My take: retinoids, vitamin C, and sunscreen have far stronger evidence for skin aging. If hormonal skin changes are part of a broader estrogen conversation, that's a good reason to assess your hormone status comprehensively.
Practical notes on estrogen cream
- Vaginal estrogen cream doesn't need progesterone. Because absorption is local and minimal, you generally don't need a progestogen to protect the endometrium — unlike systemic estrogen in women with an intact uterus.
- Transfer risk with topical cream. Skin contact before drying can transfer estrogen to partners or children. Let it dry completely, then cover the area.
- Dose consistency matters. Unlike patches, creams require measuring the same amount every time to maintain stable hormone levels.
- The FDA black box warning doesn't apply to vaginal estrogen cream. It was derived from systemic hormone trial data.
- Breast cancer history isn't an automatic disqualifier. Many oncologists approve low-dose vaginal estrogen cream for survivors with severe GSM. This is a nuanced, individualized decision - not a blanket no.
How estrogen cream fits into a full hormone plan
Estrogen cream is one of several hormone replacement therapies. Some women do well on topical estrogen cream alone for systemic relief. Others combine vaginal estrogen cream for local symptoms with a patch for systemic coverage, plus progesterone. Some women's hormone picture also involves testosterone, thyroid, cortisol, or other factors - which is why BHRT at Clarus Health starts with 150+ biomarkers, not a symptom checklist.
If you've been managing estrogen on your own, or if a previous provider dismissed your hormone questions, you can also explore how other therapies like stellate ganglion block — which directly addresses the hot flash pathway — or NAD+ therapy fit into the larger picture of how you feel. Hormones rarely exist in isolation.
Schedule a free consultation to talk through your hormone health with our team.

Anthony Kaveh MD
Dr. Kaveh is a Stanford and Harvard-trained anesthesiologist and integrative medicine specialist. He has over 1,000,000 followers on social media and has guided hundreds of patients throughout transformative healing experiences. He is an authority on Ketamine, NAD, SGB, and genomics-guided therapies. He is a continuing medical education lecturer in the Bay Area.


